Carpal Tunnel Syndrome (CTS) is a common condition that arises from the compression of the median nerve as it passes through the carpal tunnel in the wrist. This nerve compression can lead to a range of symptoms, significantly affecting hand function and quality of life.
Understanding the Median Nerve
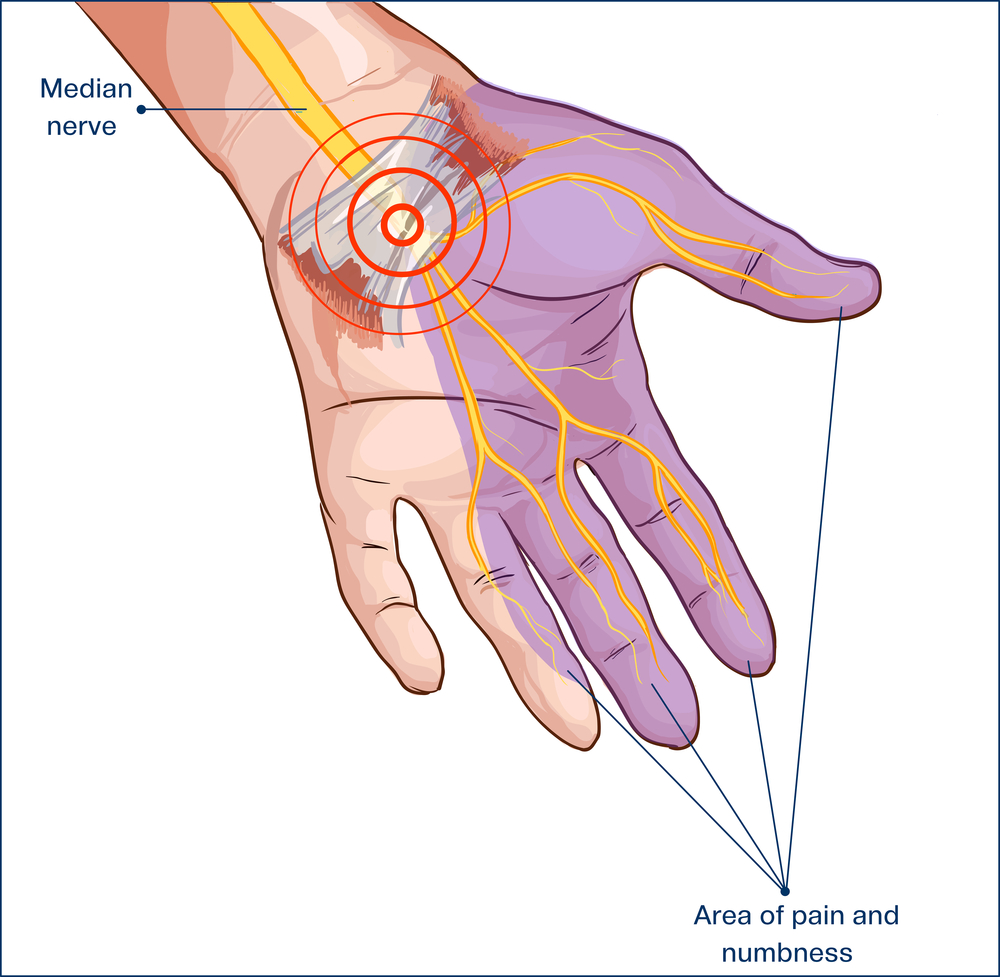
The median nerve is crucial for the sensory and motor functions of the thumb and first three fingers. It originates from a network of nerve roots in the neck, travels down the arm, and passes through the carpal tunnel at the wrist. The carpal tunnel is a narrow passageway surrounded by bones and ligaments. If any swelling occurs in this area, it can pinch the median nerve, leading to CTS.
Symptoms of Carpal Tunnel Syndrome
The hallmark symptoms of CTS include:
- Numbness or tingling in the thumb, index, middle, and part of the ring fingers
- Occasional shock-like sensations that radiate to these fingers
- Pain and discomfort in the wrist and hand, which may extend up to the arm
- Weakness in the hand and difficulty grasping objects
These symptoms often worsen over time and can be more pronounced during the night.
Causes and Risk Factors
Several factors can contribute to the development of CTS:
- Repetitive hand and wrist motions
- Genetic predisposition
- Hormonal changes, such as those during pregnancy
- Health conditions like diabetes, rheumatoid arthritis, and thyroid gland imbalance
- Prolonged exposure to vibratory tools
Diagnosing Carpal Tunnel Syndrome
Diagnosis typically involves a physical examination and may include:
- Tinel’s test, where tapping over the median nerve elicits symptoms
- Phalen’s test, where flexing the wrist for 60 seconds produces symptoms
- Electromyography and nerve conduction studies to assess the electrical activity of muscles and nerve health
Treatment Options
Treatment strategies for CTS vary based on the severity of the symptoms and can include:
Conservative Treatments
- Wrist splinting, especially at night, to alleviate symptoms
- Anti-inflammatory medications or corticosteroid injections to reduce inflammation
- Physical therapy and exercises to strengthen the wrist and hand muscles
Surgical Treatments
For severe cases, surgery may be necessary to relieve pressure on the median nerve. The most common procedure is called carpal tunnel release, which involves cutting the ligament that forms the top of the tunnel on the palm side of the hand to lessen the pressure on the median nerve.
Prevention and Management
Preventive measures can significantly reduce the risk of developing CTS:
- Regular breaks during repetitive tasks
- Proper hand and wrist position
- Exercises to stretch and strengthen the wrist and hand muscles
- Ergonomic adjustments in the workplace, such as using a suitable keyboard and mouse
Carpal Tunnel Syndrome is a treatable condition, but early diagnosis and appropriate management are crucial to prevent long-term damage to the median nerve. If you experience symptoms of CTS, it’s important to seek medical advice early to explore treatment options suitable for your specific condition.
References
